
Table of contents
Aseptic processing has always been one of the most closely watched areas in pharmaceutical manufacturing. Regulatory expectations have only sharpened since the revised EU GMP Annex 1 took effect, raising the bar on contamination control and barrier technologies. But knowing the rules have gotten stricter is one thing, and having visibility into where facilities are actually getting cited and what happens next is another.
Using Redica's global inspection and enforcement database, we analyzed compliance findings from 2022 to present across FDA, EMA/MHRA, and PIC/S member agencies. The data points to a consistent and consequential pattern: sterility observations are among the most frequently cited findings, and they are also among the most likely to escalate.

Sterility observations punch above their weight
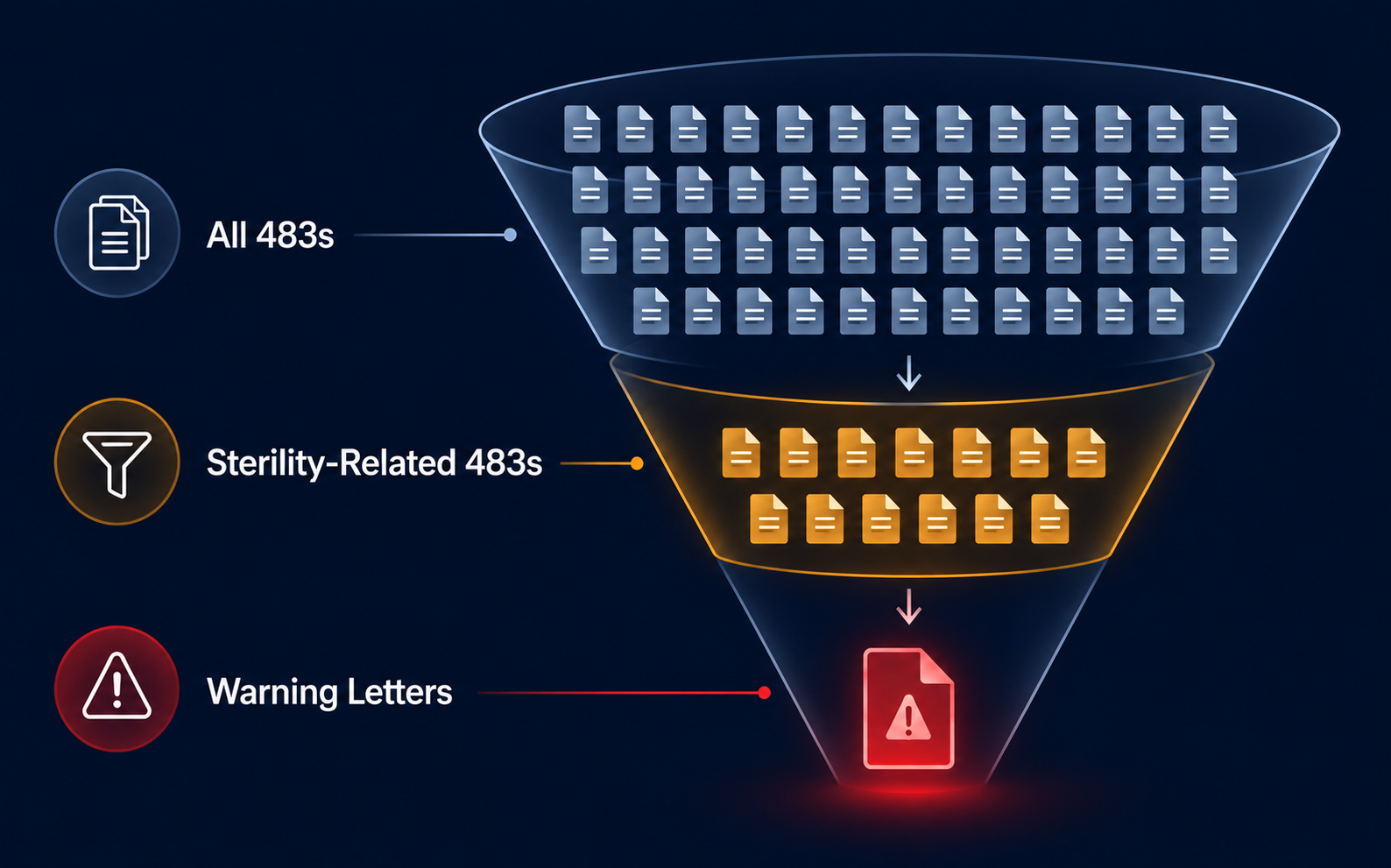
When in doubt, start with the volume. Since 2022, sterility-related issues have accounted for 8% of all 483 observations and 42% of production-specific observations across 2,407 human drugs GMP 483s. That concentration alone signals a persistent compliance challenge, but the number that should really command attention is that 37% of 483s that escalated to a Warning Letter cited sterility issues.
For any facility that receives a 483 with sterility findings, that escalation rate should directly inform how quickly remediation gets prioritized.
Where the findings cluster
Drilling into the sterility observation data reveals two main 483 categories. Microbiological contamination accounts for 64.2% of citations, followed by environmental monitoring at 20.0%. The remainder covers smoke studies, method accuracy, media fills, and personnel monitoring.
Six compliance challenge areas drive the bulk of these findings:
- Aseptic technique and personnel behavior tops the list, covering exposed skin during filling operations, insufficient glove disinfection, rapid movements that disrupt ISO 5 airflow, and unqualified interventions. These are foundational requirements, and they continue to generate citations regularly.
- Facility design and cleanroom integrity generates findings around inadequate HEPA coverage, incorrectly positioned particle counters, insufficient pressure differentials, and airflow turbulence near open product.
- Environmental monitoring programs draw scrutiny when sampling sites lack justification, when recurring mold excursions go uninvestigated, when incubation practices are inadequate, or when surface monitoring is missing altogether.
- Sterilization and disinfection gaps include absent disinfectant efficacy studies for filling equipment, validation gaps for classified areas, and in some cases visible residue left in cleanrooms.
- Contamination investigations and CAPA failures surface when OOS microbial or endotoxin results are not investigated to root cause, or when recurring excursions receive superficial responses rather than substantive corrective action.
- Media fill deficiencies arise when simulations are not conducted under worst-case conditions, when interventions are treated as routine rather than scrutinized, or when equipment used in actual production is excluded from the simulation entirely.
Predicting Warning Letter risk
Redica's proactive inspection readiness model estimates your Warning Letter risk following 483 issuance, and it’s validated against historical outcomes across thousands of inspections. SHAP analysis identifies the factors driving elevated risk scores, and sterility observations sit at the top of that list.
The risk scales not just with whether sterility was cited, but with how many times sterility was cited within an inspection. Other high-weight factors include for-cause inspection designation, repeat observations, expert inspector assignment, and above-average observation counts overall. After receiving a 483, facilities can use these risk signals to direct remediation resources toward the areas carrying the highest risk, rather than wasting resources treating every finding as an equal priority.
Annex 1 has raised the bar on contamination control
The 2022 Annex 1 revision established the Contamination Control Strategy as a standard regulatory expectation, not an optional documentation exercise. MHRA inspectors are now actively citing CCS deficiencies at sterile sites, and the inspection history makes clear that just having a CCS in place is no longer enough.
Three patterns stand out in recent MHRA findings. The first is scope gaps: CCS documents that address cross-contamination while omitting other Annex 1-required elements. The second involves gowning requirements, specifically at sites that have not addressed additional protective measures such as facemasks in Grade C and D areas during contamination-risk activities. The third, and most telling, concerns the quality of the underlying risk logic.
In one 2022 MHRA inspection, a CCS was cited because it had scored cross-contamination detection as high despite relying on tests such as pH, conductivity, and osmolality that may not be sensitive enough to detect contamination reliably. That finding demonstrates a meaningful shift in inspector expectations that the document now must not only exist and cover the required elements, but also hold up to scrutiny on the logic itself.
What this means for compliance teams
Taken together, the enforcement record points to a clear prioritization signal for quality and regulatory professionals. Sterility citations are overrepresented in Warning Letter escalations, carrying disproportionate risk relative to their share of total observations. Aseptic technique and environmental monitoring remain the most persistent challenge areas. Risk models offer a structured way to act on inspection outcomes before enforcement follows. And Annex 1 has established a new baseline for what a defensible contamination control strategy requires in practice.
For organizations operating sterile manufacturing sites, the data makes it clear that aseptic processing compliance now requires being treated as a standing risk management priority, not a reactive one. See for yourself how Redica's inspection data and risk modeling can help your team identify and prioritize sterility compliance gaps with a free demo!



